GI Physiology Unit
Established in 1994, the GI Physiology Unit is now recognised internationally as one of the premier clinical and research centres in the field of functional gastrointestinal disorders. The clinical service, which supplies the resources for aligned research, currently provides for more than 2,500 patients per year. The Unit presently boasts 20 full-time and affiliated staff members, including eight clinical research fellows working toward higher degrees. Co-Directors of the Unit are Dr Mark Scott (colorectal) and Professor Daniel Sifrim (upper GI).
Five clinical / research laboratories are available (two upper GI and 2 lower GI - incorporating a dedicated x-ray facility, and a gamma camera suite, see below), enabling a comprehensive range of investigations, covering the entire GI tract, to be carried out.
Upper and mid GI
Standard oesophageal manometric trace, using an 8 channel catheter: the upper 4 channels are spaced 5cm apart, and clearly show propagation of three oesophageal contractions during swallowing. The lower 4 channels represent radially arranged ports located within the lower oesophageal sphincter.
Tests available:
- Standard oesophageal manometry
- High resolution oesophageal manometry
- 24-hour ambulatory oesophageal pH measurement
- 24-hour ambulatory multichannel oesophageal impedance and pH measurement
- Tests of oesophageal chemo- and mechanosensitivity
- Electrogastrography
- Ambulatory small bowel manometry
- Sphincter of Oddi manometry
- Oesophageal transit
- fluoroscopic
- scintigraphic
- Scintigraphic gastric emptying
- Cholescintigraphic hepatobiliary iminodiacetic acid (HIDA) scan for gallbladder / biliary function
- Multi-purpose breath testing analysis for gastric emptying, orocaecal transit, lactose intolerance, small bowel bacterial overgrowth and Helicobacter pylori
Lower GI / anorectal
Tests available:
- Standard anal manometry
- Rectal sensitivity testing
- thermosensitivity
- mechanosensitivity
- electrosensitivity
- Electrophysiological assessment
- pudendal nerve function
- anal sphincter EMG
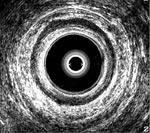
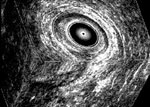
- 2-D and 3-D endo-anal and endo-rectal ultrasonography
- Ambulatory rectosigmoid manometry
- Pancolonic manometry
- Single or dual barostat evaluation of colorectal sensorimotor function and reflexes
- Evacuation proctography
- barium
- Colonic transit studies
- radio-opaque marker
- scintigraphic
- wireless capsule technology
Anorectal procedures (below): (left) 6-channel solid-state rectosigmoid manometry catheter in situ; (middle) 2-D endo-anal ultrasound representation of the anal sphincters in a normal volunteer; (right) 3-D representation of the anal sphincters in a patient with fistula-in-ano